
By Matthew Holt
If the health policy believes something, it is a good thing that primary care is a good thing. In theory we should all have strong relationships with our doctors for primary care. Through the health system they have to navigate and arrive at our door like Marcus Welby MD when needed. Wonks such as I believe that if you introduce such a relationship that patients will receive preventive care, get the right medicines and take them, avoid first aid and have fewer hospital admissions – as well as much less costs. In general, that is the theory behind HMOs and their descendants on the last days, on value -based care and ACOs
Of course there are decent examples of system -based systems based on first -line, such as the British NHS or even Kaiser Permanente or the Alaskan Artic Slope Native Health Association. But for most Americans that is a fantasy country. Instead, we have a system where primary care is the ugly stepchild. It is slowly thrown through and picked apart. Even the Walmart’s wealth could not let it work.
There have been at least 3 types of first -line care in recent decades. And none of them is really successful in making that “first -line care as the lynchpin of the health of the population”.
The first is the first -line doctor who is purchased by and/or works for the large system. The point of these practices is to ensure that references for the expensive things go to the right hospital system. For a long time, those first-line doctors have lost their employers moneyBob Kocher said $ 150-250k per year per doctor in the late 2000s. So why are they stored by the larger systems? Because the patients they allow in the hospital are insanely profitable. To consider This NC system that ultimately cleared the large hospital system Atrium Because they only wanted the references. As you would expect, the benefits of primary care of first -line care are difficult to find between those systems. (If you have time to watch Eric Bricker’s Video On Atrium & Troyon/Mecklenberg)
The second is urgent care. Urgent care has replaced primary care in a large part of America. The Number of urgent care centers doubled in the past decade or so. Although it has achieved some pressure from first aid, urgent care has replaced primary care because it is useful and you can easily get agreements. But it does not do population health and healthcare management. And often the urgent care centers are the property of hospital systems they use to generate references, or private equity pirates who try to stimulate costs that have no control.
Thirdly, TeleHealth, mainly associated with pharmacies, has many people able to gain access to medicines in a cheaper and more convenient way. Of course this is not really complete primary care, but HIMS & HARE and their many, many competitors provide access to common antibiotics for UTIs, contraceptive pills and also mental health drugs, as well as those boner and baldness pills.
That does not mean that there have been no attempts to build new types of primary care
Oak Street, Chenmed and Iora (now part of one medical) were built with the idea of resolving first -line care services to seniors in Medicare Advantage, with the idea that – like Kaiser and his competitors – they can take financial risk for specialty and hospital care. The theory, as the founder of Iora Rushika Fernandopulle always said, was “double the expenditure for primary care and the total costs reduced by 30%.” It is not so clear whether they have ever come there.
Of course, just like everything else in American Health Care Oak Street and Iora, repetitions of previous efforts of Mullikin, Friendly Hills, Health partners and much more were to manage the general healthcare costs by taking the risk of competent care. None of these experiments was left alone by the financial brittle long enough to see what would have happened if they happen. The stock market of the nineties and 2020s are full of cemeteries of listed primary care groups that all had promising starts. If they were left alone for long enough to grow organically, it is possible that we would see a different future. We can even see that future as absorbed health, transcarent and others to build their first -line care/telehealth/navigation/navigation/centers of excellence. But it will take a while
In general, risky first -line care remains a lonely company, despite the fact that it has been the desired policy resource solution since Sydney Garfield began to pay in advance of employees on the Grand Coulee Dam in 1933
Of course you can, because you can still get excellent primary care, it will just cost you.
Silicon Valley Multi-Millionaires Pay Jordan Shlain’s private medical medical $ 40ka year plus for white manual service. On the other side of the scale, one medical $ 80-200 a year collects from patients who pay for access to appointments from the next day, NPs who actually answer e-mails and a free TeleHealth service for urgent care. In the meantime, a whole series of doctors who have opted for the hassle of invoicing insurers and to charge for caretaker care between $ 500 and $ 5000 per year. Then there are a lot of first -line services that use TeleHealth, home visits and NPs, often combined with clinics in the field of workplaces
Which means that the number of people who offer real Marcus Welby MD style of first -line care in the community continues to fall.
And it’s not that hard to find out why. The average primary doctor makes much less than their special counterparts.
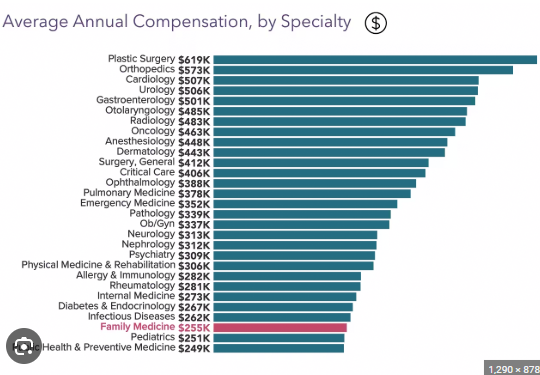
The costs for primary care are low. They are intentionally set in this way by the RUC (the relative value of the update of the value scale) is dominated by specialists and essentially establishes medicine costswhich are then followed by most private insurers. So most doctors tend to look at the upper end of this graph instead of the bottom, they choose their residence slots. American health care is expensive because we have too many specialists who do useful care marginal, and too many hospitals (and pharmaceutical and device companies) that remove the bank. And it is all related to that graph.
There was a rather strange count of Kff that said Almost 50% of American doctors were in first -line careBut that had many doctors his ‘first -line care’ who do not offer traditional primary care. This is of course wrong, but it gives a hint for the solution.
There are 340 million Americans. We can give everyone a PCP and place them in a panel of 600 people (in contrast to the 2-3,000 typical PCP panel. That number happens to be something MDVIP and other caretaker service offer. That would require 570 thousand PCPs. That is about 60% of doctors after the residence in America.
So if we have converted all those currently licensed PCPs and the addition of NPs, we could provide everyone in America caretaker style. Those doctors would be immediately available and help their patients by navigating the system.
The proponents believe that caretaker -medicine is not only better, but is also much cheaper than regular care. MDVIP claims it saves $ 2500 per patient Even after paying his doctors more, which is about 20% of health expenditure. My claim is that we can give every PCP $ 2K per patient (or $ 1.2 million per 600 patient panel), of which they could use $ 300-500k to run their practice, and they could keep $ 700k to pay themselves.
So my proposal is that we really give everyone high-end first-line care, pay first-line care very well and save a boot load money. And apparently we have almost enough first -line care documents to do it. If they were paid at least $ 700k a year, we would soon find much more of it.
Matthew Holt is the publisher of THCB
#repair #paradox #primary #care #health #care #blog